A coronary calcium score is a low-dose CT measurement of calcified plaque in the heart arteries. A score of 0 means no calcified plaque was detected; higher scores indicate a greater burden of coronary atherosclerosis and higher future cardiovascular risk. The test is most useful in people without symptoms, when the result could change a decision about preventive treatment — usually whether to start or intensify cholesterol-lowering therapy.
What do calcium score results mean?
Scores are reported in Agatston units (AU). The bands below are the ones used in routine Australian practice. What matters is not only the number but how it compares with others of the same age and sex.
| Score (AU) | Plaque burden | What it usually means |
|---|---|---|
| 0 | None detected | No calcified plaque. Low short-term event risk, and in Australian guidance this can reclassify selected people to low risk. It does not exclude non-calcified plaque. |
| 1–99 | Mild | Atherosclerosis is present. Management depends on the wider picture — age, LDL-cholesterol, family history, Lp(a), diabetes, smoking. |
| 100–299 | Moderate | Established atherosclerosis. Generally supports lipid-lowering therapy and firm risk-factor control. |
| 300–999 | Extensive | High burden. Event rates in this range approach those of people with established cardiovascular disease.3 |
| ≥1000 | Very high | Very large calcified plaque burden. Intensive prevention is warranted; the score itself does not indicate whether any lesion is obstructive. |
A score of 100 may not be unusually high for a 75-year-old man, but it still represents coronary atherosclerosis; the same score would be markedly premature in a 45-year-old woman. Australian guidance is explicit on this: a score above 99 AU or at or above the 75th percentile for age and sex may reclassify someone to high cardiovascular risk, while a score of 0 may reclassify them to low risk.1 Always ask for both figures.
CAC percentile calculator
Where a score sits relative to others of the same age and sex — the figure that tells you whether the burden is expected or premature.
MESA coronary calcium risk calculator
Folds a measured CAC score into a 10-year coronary heart disease estimate alongside the standard risk factors.
- What the results mean
- What the test actually measures
- Who should — and should not — have one
- The scan, radiation, preparation and cost
- What happens after the result
- Limitations, and why zero is not a guarantee
- Calcium score vs CT coronary angiogram
- Where CAC fits in Australian risk assessment
- Coronary calcium in athletes
- Watch
- Frequently asked questions
- References
What the coronary calcium score actually measures
Atherosclerosis is an inflammatory process in the arterial wall that typically begins decades before symptoms. Plaque is usefully described in three forms: non-calcified, mixed or partially calcified, and calcified. Calcification generally develops as plaque matures, so calcium is a marker that atherosclerosis is established rather than a measure of how dangerous any individual lesion is.
A coronary calcium scan is a non-contrast, ECG-gated CT of the heart. Software identifies calcified areas within the coronary arteries and converts their area and density into an Agatston score. Higher scores track with higher rates of future myocardial infarction, coronary death and stroke.45 The scan tells you whether disease is present and roughly how much — not whether any artery is narrowed.


Who should have a calcium score — and who should not
I order a calcium score when the result is likely to change a prevention decision — usually whether to start or intensify lipid-lowering treatment in someone whose risk sits in the middle and who is undecided. I do not use it to investigate chest pain, to monitor response to a statin, or to decide on angiography in isolation.
The single organising principle is that a calcium score is worth doing when the result would change what happens next.
- Adults without symptoms whose calculated risk is intermediate
- People genuinely undecided about starting or intensifying lipid-lowering therapy
- Risk that the standard factors do not fully explain — strong family history of premature coronary disease, elevated Lp(a), or discordance between LDL-C and the overall clinical picture
- Anyone with cardiac symptoms — the question is diagnosis, not risk, and stress echocardiography or CT coronary angiography answers it
- Already clearly high risk — intensive prevention is indicated regardless of the score
- Established cardiovascular disease, or already on well-adhered lipid-lowering therapy at target
- Very low risk, where the result will not alter management
In practice the yield is greatest between roughly 45 and 75 years of age. Below 40, calcium has often not had time to deposit even where plaque exists, so a score of zero carries less reassurance — particularly in familial hypercholesterolaemia or high Lp(a). A high score in a young person is the opposite: always significant, and should prompt firm treatment. In older adults, some calcification is common, which is exactly why the percentile matters more than the raw number.
A high score can move a borderline picture into one that clearly requires treatment. The reverse does not hold: a low or zero score does not convert a high-risk patient into a low-risk one.
The scan, radiation, preparation and cost in Australia
The scan itself takes a few minutes on the table, with a total appointment of around 15–20 minutes. There is no contrast dye, no cannula and no exercise component. You lie flat, ECG leads are attached, and images are acquired during a single breath-hold.
Preparation
Preparation is usually minimal, but follow the imaging centre’s own instructions — some ask you to avoid caffeine or smoking beforehand, because a slower, more regular heart rate improves image quality. Take your usual medications as normal unless told otherwise.
Radiation and pregnancy
A modern calcium score scan delivers roughly 1 mSv, comparable to a few months of natural background radiation and considerably less than a diagnostic chest CT. It is not performed in pregnancy: calcium scoring is an elective risk-refinement test with no urgency, so it is deferred. If there is any possibility of pregnancy, tell the radiographer before the scan.
Incidental findings
The scan includes part of the lungs, aorta, spine and upper abdomen. Incidental findings — most commonly small lung nodules — are reported in a minority of scans. Most are benign, but some generate follow-up imaging. This is a real, if modest, cost of testing and a reason not to scan people for whom the result will not change management.
Cost and Medicare
There is no Medicare Benefits Schedule item for coronary calcium scoring in Australia, so the scan is not bulk billed and is paid out of pocket. Fees vary between providers; most Sydney practices quote somewhere in the vicinity of $100–$250. Confirm the fee with the imaging centre when booking, and ask whether the report will include the age- and sex-matched percentile.
What happens after the result
The score is not the endpoint — the decision it informs is. A worked example makes the logic concrete.
A 55-year-old man has mildly elevated LDL-cholesterol, well-controlled hypertension, no smoking history and no family history he considers alarming. His calculated risk is intermediate, and he is reluctant to start a statin.
His calcium score returns at 300. He is no longer someone with borderline numbers; he is someone with demonstrable coronary atherosclerosis, and more intensive LDL-C lowering is clearly justified — see the 2026 dyslipidaemia guideline summary for targets, and the unit converter if results are reported in mg/dL.
Had the score been zero, the conversation would have been different but not automatically reassuring: a zero result supports a more individualised discussion provided there is no very high LDL-C, familial hypercholesterolaemia, diabetes or markedly elevated Lp(a).
Two further points about what follows a result. First, aspirin is not an automatic consequence of a high score — that decision rests on overall cardiovascular risk weighed against bleeding risk. Second, a high calcium score should not by itself lead to invasive coronary angiography in an asymptomatic person. That practice causes harm and is not recommended.

Limitations, and why zero is not a guarantee
Calcium scoring is a risk-stratification tool. It is not a diagnostic test, and it is the wrong instrument for a patient who is already high risk or who has cardiac symptoms.
It does not see non-calcified plaque
The scan measures calcium. Non-calcified plaque — lipid-rich, often younger, and the type most implicated in acute events — is invisible to it. A person can have a substantial, even flow-limiting, non-calcified lesion and a calcium score of zero.

It says nothing about whether a lesion is obstructive
A calcium score neither defines stenosis severity nor establishes whether any lesion causes ischaemia. Someone can have a score above 500 with entirely non-obstructive disease and preserved perfusion, or a score of zero with a critical stenosis. Where the clinical question is ischaemia, the answer comes from functional or anatomical imaging — stress echocardiography, CT coronary angiography or invasive angiography.
False reassurance is the main clinical hazard
This is the limitation that causes real harm. In symptomatic or high-risk people, a zero score gets read as an all-clear — and treatment is declined, deferred or abandoned on the strength of it.
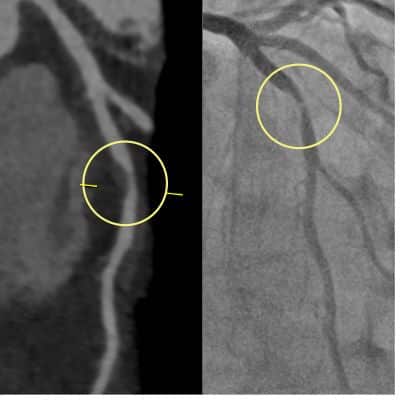
A 44-year-old man, smoker, with hypercholesterolaemia and a strong family history of premature ischaemic heart disease, presented with chest pain. He had a satisfactory stress test and a calcium score of zero, and was reassured. Symptoms persisted; CT coronary angiography demonstrated a significant mid-LAD stenosis, confirmed at invasive angiography — entirely non-calcified, hence the score of zero. He proceeded to angioplasty and stenting.
A second case with the same error
A 37-year-old man presented with breathlessness and throat discomfort on exertion. He had hypertension, hypercholesterolaemia, prediabetes and a sedentary lifestyle. A calcium score was ordered and returned zero, which produced a false sense of reassurance and led him to decline medical therapy.
Symptoms persisted. A stress echocardiogram and CT coronary angiogram subsequently demonstrated severe proximal LAD disease requiring stenting. In both this case and the one above the error was identical: a risk-stratification test was used to answer a diagnostic question.


A calcium score of zero lowers risk at a population level. It does not exclude obstructive coronary disease in an individual with symptoms or strong inherited risk. Interpret it alongside history, lipid markers, Lp(a) and sometimes ApoB — never as a stand-alone answer.
Calcium score vs CT coronary angiogram
These are different tests answering different questions. A calcium score estimates risk in someone without symptoms. A CT coronary angiogram (CTCA) is a diagnostic test that visualises plaque, the vessel lumen and anatomical narrowing. CTCA does not directly measure blood flow or ischaemia unless combined with CT-FFR or perfusion imaging.
| Calcium score | CT coronary angiogram | |
|---|---|---|
| Question answered | How much calcified plaque is present, and what does that mean for future risk? | Is there a narrowing, where is it, and how severe does it look? |
| Typical patient | Asymptomatic, intermediate risk, treatment decision uncertain | Symptomatic, or abnormal functional testing, or pre-operative assessment |
| Contrast | None | Iodinated contrast; cannula required |
| Non-calcified plaque | Not detected | Detected and characterised |
| Radiation | Around 1 mSv | Varies with scanner and protocol; modern prospectively gated studies can approach calcium-score doses, while retrospectively gated protocols are substantially higher |
| Ischaemia | Not assessed | Not directly assessed unless CT-FFR or perfusion is added |

Why not simply do a CTCA instead?
CTCA gives more information, but in the asymptomatic setting there are sound reasons to prefer a calcium score: it is simpler, usually lower-dose, requires no contrast — which matters in kidney impairment or contrast allergy — costs less, and is less likely to generate incidental coronary findings that do not change management. CTCA in an asymptomatic person frequently identifies non-obstructive plaque that generates anxiety and further testing without changing the plan, which remains intensive medical therapy and lifestyle change either way.
In symptomatic patients, or where high-risk features are present, CTCA is the appropriate test. The choice rests on symptoms, risk profile and clinical judgement rather than on which scan yields more images.
Where CAC fits in Australian risk assessment
In Australia, the starting point for someone without known cardiovascular disease is the Australian CVD risk calculator, which estimates five-year risk of a cardiovascular event and sorts people into low, intermediate and high categories. A calcium score is not a screening test that sits alongside it — it is a reclassification tool used when the calculated result leaves the treatment decision genuinely unresolved.
The Heart Foundation position statement sets out how that reclassification works: if calcium scoring is undertaken, a score of 0 AU may reclassify a person to low absolute risk, and a score above 99 AU or at or above the 75th percentile for age and sex may reclassify them to high absolute risk — in both directions, informed by discussion rather than applied mechanically.1
The 2026 ACC/AHA dyslipidaemia guideline positions the PREVENT equations as the preferred risk model for adults aged 30–79 in the United States, with selective calcium scoring, Lp(a) and ApoB used to refine the estimate.2 PREVENT is a well-validated, race-free model that also incorporates kidney and metabolic variables, and it is useful for cross-checking — but it reports 10- and 30-year risk against US thresholds, not the five-year categories Australian practice is built around. Read it as a supplement to Australian risk assessment, not a replacement for it. Our 2026 guideline summary covers the differences.
Alongside imaging, two blood markers add information that standard panels miss. Lp(a) identifies inherited risk that risk calculators systematically underestimate, and should be measured at least once in adult life. ApoB counts atherogenic particles directly and is more informative than LDL-C where triglycerides are raised or metabolic syndrome is present. Risk estimation, inherited markers, particle count and imaging each answer a different question; together they give a far clearer picture than any one of them alone.
Coronary calcium in athletes
Masters endurance athletes have a higher prevalence of coronary calcification than sedentary controls, and the plaque phenotype is more often calcified rather than mixed or non-calcified.9 This is a genuine and repeatedly observed finding, and it is also the one most often over-interpreted.
Any coronary calcium represents coronary atherosclerosis. Training may influence plaque composition and, plausibly, prognosis for a given burden — it does not neutralise the finding or make it a benign variant. An athlete with a calcium score of 200 has coronary artery disease, and LDL-C, blood pressure, Lp(a) and family history should be addressed on that basis.
What the athletic context reasonably changes is tone, not treatment. CAC alone is not an indication to stop training. Symptoms or other high-risk features, however, warrant clinical assessment before continuing vigorous exercise. Overall risk may still be low where the lifestyle is healthy and no other major risk factor is present — but that is a judgement made after the risk factors have been examined, not a reason to skip examining them.
Watch
Frequently asked questions
Is a calcium score of 0 good?
Yes, in the right person. A score of zero means no calcified plaque was detected and is associated with low short-term event risk; in Australian guidance it may reclassify selected people to low risk. It is less reassuring in adults under 40, in familial hypercholesterolaemia, in markedly elevated Lp(a), and in anyone with cardiac symptoms — because non-calcified plaque is invisible to the scan.
Is a calcium score of 100, 300 or 400 dangerous?
None of these numbers describes an immediate danger; they describe accumulated disease and elevated future risk. A score of 100–299 indicates established atherosclerosis and generally supports lipid-lowering therapy. Above 300, event rates approach those seen in people with known cardiovascular disease, so prevention should be intensive. A score of 400 sits in that band. None of these figures tells you whether an artery is narrowed, and none is a reason for angiography in someone without symptoms.
What is a normal calcium score for my age?
There is no single normal figure, because expected calcium rises steeply with age. Zero is optimal at any age. Beyond that, the meaningful comparison is the age- and sex-matched percentile: at or above the 75th percentile is considered high, regardless of the absolute number. The percentile calculator gives that figure.
How much does a calcium score cost in Australia, and is it covered by Medicare?
There is no Medicare item number for coronary calcium scoring, so it is not bulk billed and the full fee is out of pocket. Costs vary by provider, commonly in the range of about $100–$250 in Sydney. Confirm the fee when booking and ask that the report include the age- and sex-matched percentile.
Can a calcium score be reduced or reversed?
No. Coronary calcification is essentially irreversible, and the score generally rises over time. This is not the measure of whether treatment is working — calcium scores can increase after starting a statin, and serial scanning is not a treatment-monitoring test. What treatment changes is event risk, tracked through LDL-C, blood pressure, glycaemic control and smoking status.
Should the test be repeated?
Usually not. If the score is high, the question is already answered and attention belongs on risk-factor control. Repeating it will not add information that changes management. In selected people with a score of zero — typically younger adults with some risk factors who chose against medication — a repeat at around five years is reasonable.
Do I still need a calcium score if I am already taking a statin?
Generally no. If you are taking it consistently and LDL-C is at target, the score will not change what you do. Where adherence is uncertain or LDL-C remains well above target, a score can be useful in framing the conversation about intensifying therapy — but it is being used to inform a decision, not to check the drug is working.
Does a CT coronary angiogram include a calcium score?
Many centres report it automatically, but not all. If both are wanted, ask that the calcium score be specifically requested on the referral. Note that where contrast has already been given, a separate non-contrast acquisition is needed to score calcium properly.
Is a calcium score useful in athletes?
It can be, but the result needs careful interpretation. Endurance athletes more often have calcified rather than non-calcified plaque, so a given score may carry a different prognosis than the same score in a sedentary person. That does not make the finding benign: any calcium means atherosclerosis, and the standard risk factors should be assessed and treated on their merits.
- A calcium score measures calcified plaque. It shows whether atherosclerosis is established and roughly how much — not whether an artery is narrowed.
- Read the absolute score and the age- and sex-matched percentile together. Above 99 AU or at or above the 75th percentile reclassifies to high risk; zero may reclassify to low.
- It earns its place when the result would change a prevention decision — almost always whether to start or intensify lipid-lowering therapy.
- It is the wrong test for chest pain, for monitoring treatment, and for anyone already clearly high risk.
- Zero does not exclude non-calcified plaque. In symptoms or strong inherited risk, clinical context outranks the score.
- There is no Medicare rebate in Australia; expect an out-of-pocket fee.
Not sure whether a calcium score would change anything for you?
A preventive cardiology consultation brings together risk estimation, lipid markers including Lp(a) and ApoB, and selective imaging — so that any test ordered is one that will actually inform a decision. Consultations in English and Persian (Farsi).
Book an appointmentRelated calculators and guides
References
- Jennings GL, Audehm R, Bishop W, et al. National Heart Foundation of Australia: position statement on coronary artery calcium scoring for the primary prevention of cardiovascular disease in Australia. Med J Aust. 2021;214(9):434–439. PubMed
- Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of dyslipidemia: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2026;87(19):2624–2757. doi:10.1016/j.jacc.2025.11.016. PubMed
- Budoff MJ, et al. Coronary artery calcium and risk of cardiovascular events in patients without prior atherosclerotic cardiovascular disease. JACC Cardiovasc Imaging. 2023. PubMed
- Detrano R, Guerci AD, Carr JJ, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336–1345. NEJM
- Greenland P, LaBree L, Azen SP, et al. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004;291(2):210–215. JAMA
- Nasir K, Bittencourt MS, Blaha MJ, et al. Implications of coronary artery calcium testing among statin candidates according to American College of Cardiology/American Heart Association cholesterol management guidelines: MESA. J Am Coll Cardiol. 2015;66(15):1657–1668. JACC
- Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of coronary artery calcium score of zero and other negative risk markers. Circulation. 2019;140(16):1520–1538. PubMed
- Khan SS, Matsushita K, Sang Y, et al. Development and validation of the American Heart Association’s PREVENT equations. Circulation. 2024;149(6):430–449. PubMed
- Merghani A, Maestrini V, Rosmini S, et al. Prevalence of subclinical coronary artery disease in masters endurance athletes with a low atherosclerotic risk profile. Circulation. 2017;136(2):126–137. Circulation
- Koschinsky ML, Bajaj A, Boffa MB, et al. A focused update to the 2019 NLA scientific statement on use of lipoprotein(a) in clinical practice. J Clin Lipidol. 2024;18(3):e308–e319. PubMed