- Cardiovascular risk can develop silently for many years — a heart attack or stroke may be the first obvious sign.
- Preventive cardiology identifies that risk early, using your family history, advanced lipid testing (Lp(a), ApoB), validated risk calculators and imaging where appropriate.
- The result is a clear, individualised management plan — built with you and your GP, before an event occurs.
What does preventive cardiology mean for you?
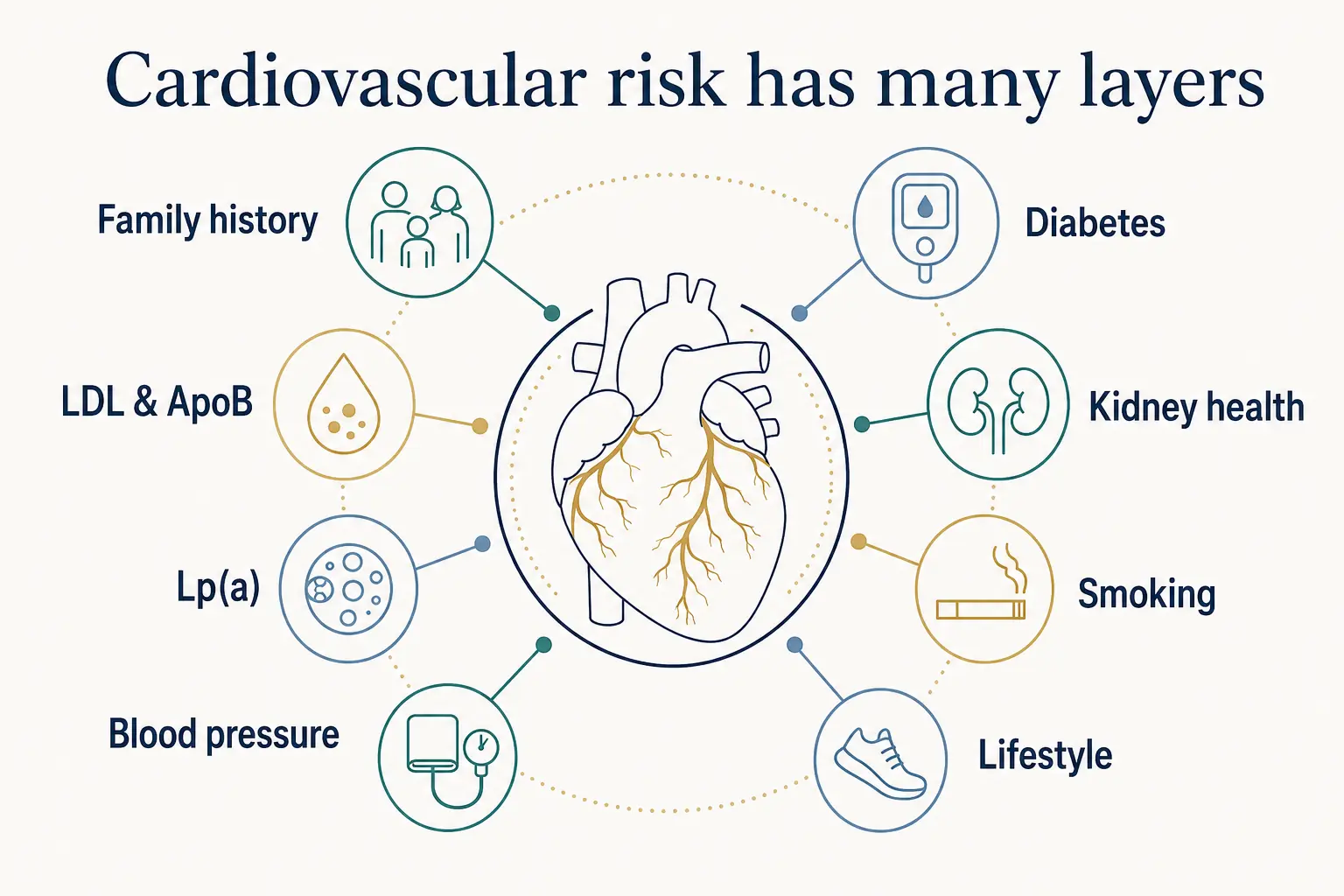
Preventive cardiology is not simply checking whether your cholesterol is "normal." It is a structured assessment of your likelihood of developing heart attack, stroke or other cardiovascular disease — and identifying which parts of that risk can be changed.
For some people, the main issue is persistently elevated LDL cholesterol. For others, risk may be driven by high blood pressure, diabetes, kidney disease, smoking or excess weight. Inherited factors such as familial hypercholesterolaemia and elevated lipoprotein(a), or Lp(a), may also increase risk even when someone follows a healthy lifestyle.
The purpose is not to predict exactly what will happen. It is to identify patterns that make cardiovascular disease more likely and determine whether earlier action could meaningfully reduce that risk. A preventive assessment may help you understand:
- Your estimated cardiovascular risk over the coming years
- Whether your family history suggests inherited risk
- Whether standard cholesterol results are telling the whole story
- Whether medication is likely to provide meaningful benefit
- Whether coronary imaging would change management
- Which lifestyle changes matter most for your particular risk profile, and what targets and follow-up you may need
Prevention does not mean performing every available test. It means selecting the information that is most likely to change what we do next.
Who may benefit from a preventive cardiology review
A preventive cardiology review may be particularly valuable when standard risk assessment does not tell the whole story. Common reasons for referral include:
A parent or sibling with heart attack, stent, bypass surgery or sudden cardiac death at a young age (men under 55, women under 65).
Persistently elevated LDL cholesterol, suspected familial hypercholesterolaemia, or difficulty tolerating statin therapy.
A raised lipoprotein(a) or ApoB result, or inherited cardiovascular risk that standard lipid panels can miss.
Newly diagnosed, difficult-to-control, or uncertain readings needing confirmation and a structured treatment plan.
Type 2 diabetes, pre-diabetes or metabolic syndrome, or chronic kidney disease (reduced eGFR or albuminuria) — all of which amplify cardiovascular risk.
An intermediate risk score, results that point in different directions, a high coronary calcium result, or wanting a specialist opinion before committing to long-term medication.
If inherited cholesterol disorders run in your family, our guides to familial hypercholesterolaemia and lipoprotein(a) explain these conditions in more detail.
What happens during a cardiovascular risk assessment?
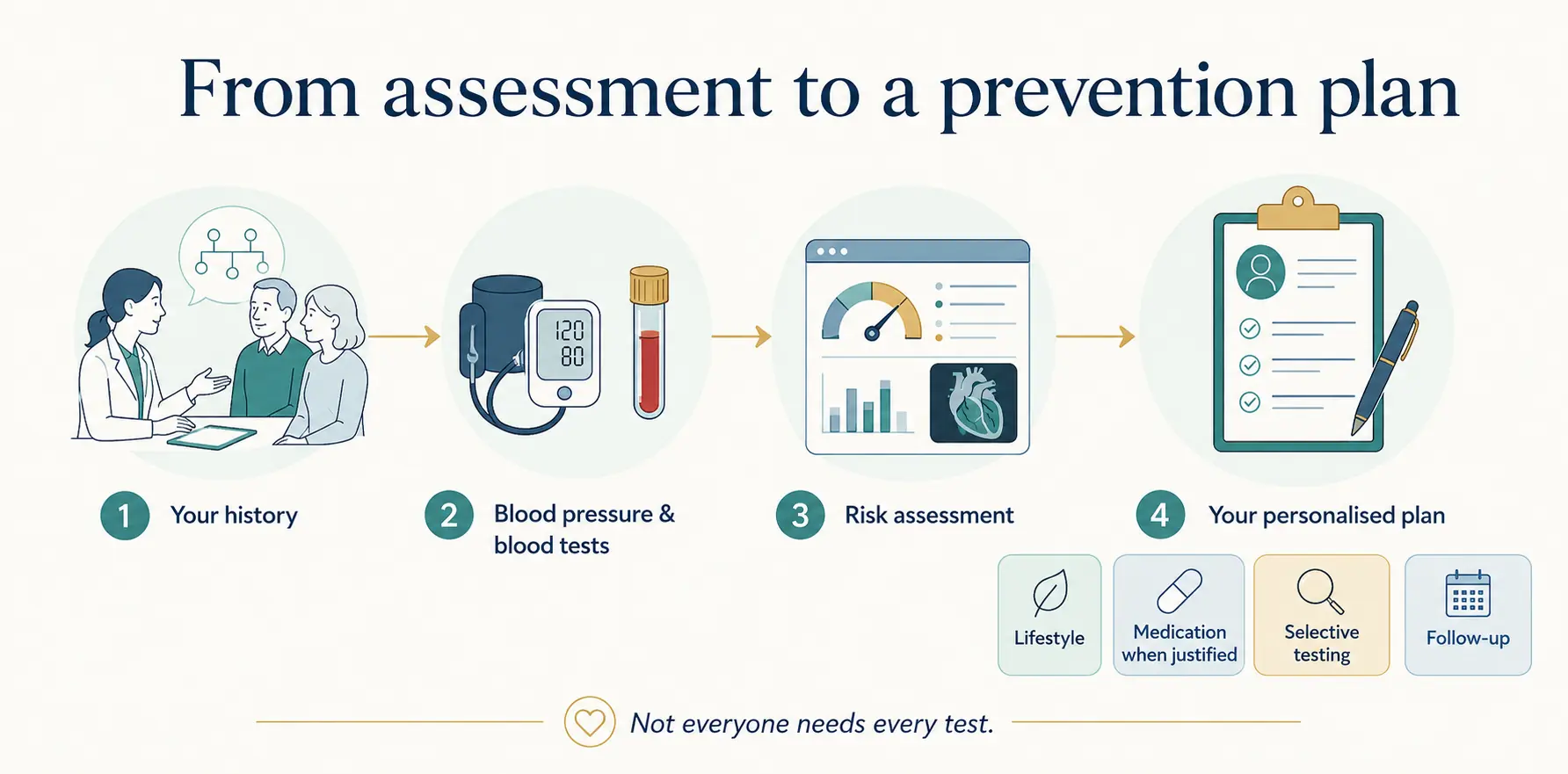
A preventive cardiology consultation begins with understanding why you are seeking assessment. Some patients have been referred because of high cholesterol or blood pressure. Others have a strong family history, an abnormal calcium score, or concern after a relative experienced a heart attack at a young age. It is a structured review rather than a quick check, and generally follows four stages:
| Stage | What happens |
|---|---|
| 1 · Understand your background | We review your personal history, family history, medications, lifestyle, blood pressure, weight and any previous cardiac investigations. The age at which cardiovascular disease occurred in relatives is particularly important. |
| 2 · Measure the important risk factors | Recent blood tests are reviewed, and additional testing may be recommended where appropriate — LDL and non-HDL cholesterol, ApoB, once-in-a-lifetime Lp(a), glucose or HbA1c, kidney function (eGFR) and urine albumin. |
| 3 · Estimate and refine your risk | For eligible adults, the Australian CVD Risk Calculator provides a useful starting point. Family history, Lp(a), ApoB or coronary calcium may refine the assessment when the calculated result does not tell the whole story; PREVENT and MESA-based estimates may add context in selected circumstances. |
| 4 · Build an individual plan | Your plan may involve lifestyle changes, treatment of cholesterol or blood pressure, additional investigation, or planned surveillance — a written plan with targets and follow-up, communicated to your GP so ongoing monitoring can continue locally. |
Many of the tools used in consultation — including the AHA PREVENT calculator and the ApoB calculator — are freely available in our cardiovascular risk calculator hub.
How might the assessment change your care?
Different people can have similar cholesterol results but require different management. For example:
- A person with mildly elevated LDL cholesterol but otherwise low risk may initially need lifestyle measures and periodic review.
- The same LDL result may carry greater significance in someone with diabetes, kidney disease, elevated Lp(a) or a strong family history.
- Very high LDL cholesterol from a young age may suggest familial hypercholesterolaemia and lead to earlier treatment and assessment of close relatives.
- An intermediate risk estimate may remain uncertain until a coronary calcium score provides additional information.
- Evidence of coronary plaque generally changes the discussion from whether prevention is needed to how intensively risk factors should be treated.
This is why treatment should not be based on one laboratory result in isolation.
What do coronary imaging results mean?
Imaging is not required for every preventive cardiology patient. It is considered when the result is likely to alter the treatment decision — typically when risk is intermediate or uncertain, or when risk estimates and family history point in different directions.
Coronary artery calcium (CAC) score. A calcium score detects calcified plaque within the coronary arteries. It can help refine risk in selected asymptomatic adults who remain uncertain about whether medication should be started. A CAC score of zero is reassuring in the appropriate clinical setting and may support deferring lipid-lowering medication in selected people after clinical review. However, it does not exclude non-calcified plaque and should not automatically override high-risk conditions such as familial hypercholesterolaemia, markedly elevated LDL cholesterol, diabetes, smoking or a strong family history of premature cardiovascular disease. A high score or high percentile reclassifies risk upward and usually shifts the discussion towards preventive therapy. Our guide to coronary calcium scoring and CAC percentile calculator explain the test in more detail.
CT coronary angiography (CTCA). CTCA provides more detailed information about the coronary arteries. It can show both calcified and non-calcified plaque and determine whether plaque is causing narrowing. It is generally considered when symptoms raise concern about coronary disease, or when anatomical information is clinically required. It is not a routine screening test for every person seeking preventive assessment.
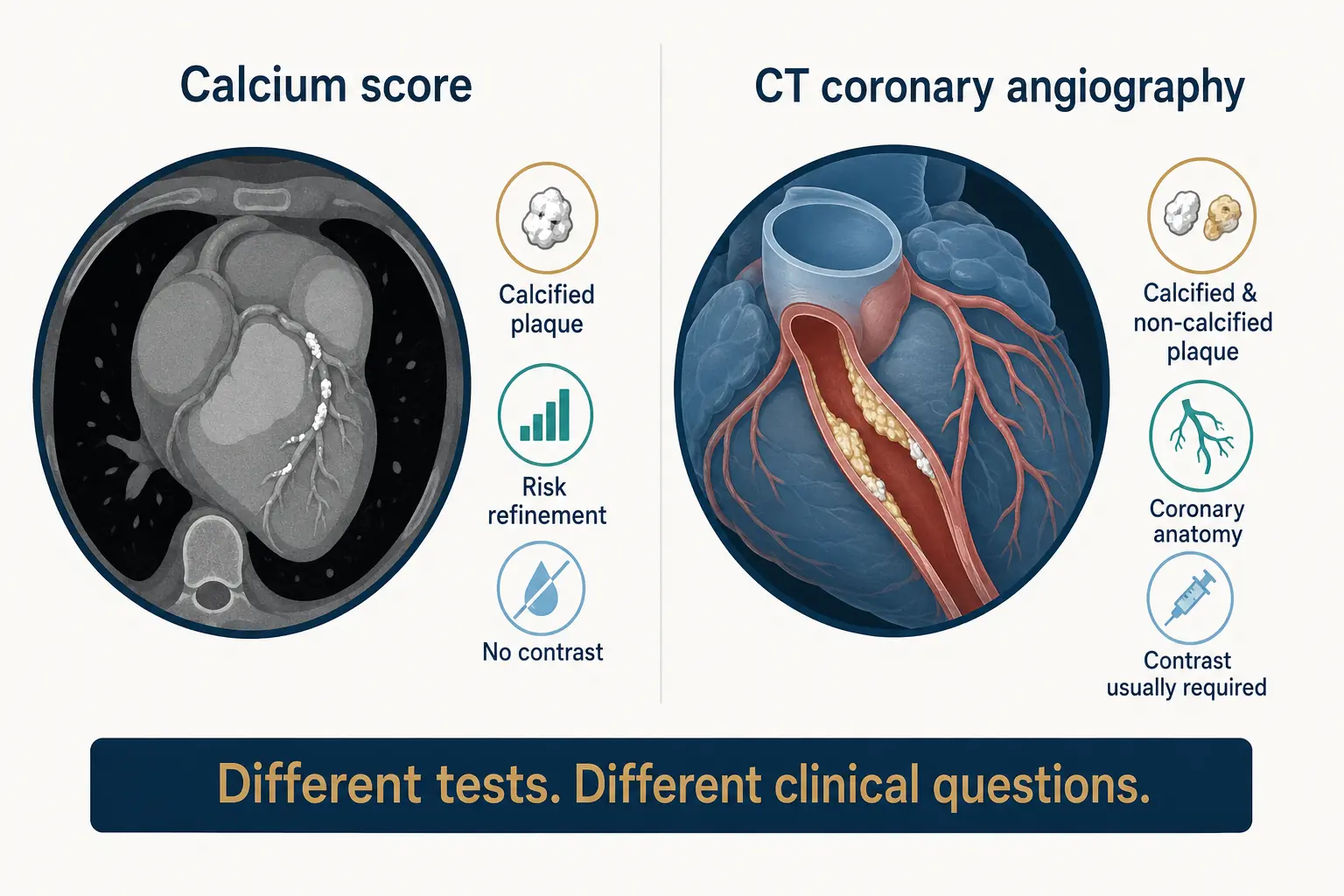
Neither test is a screening test for everyone — the right test is the one that changes what we do next.
Managing your risk
Prevention is rarely about a single number. The plan usually addresses several factors together, because their effect on risk is multiplicative.
| Risk factor | Approach |
|---|---|
| Cholesterol & ApoB | Individualised LDL and ApoB targets; statins, ezetimibe and PCSK9-pathway therapy where indicated; structured review of statin intolerance. |
| Blood pressure | Confirmation with home or ambulatory monitoring before escalating treatment; treatment to guideline targets. |
| Weight & metabolic health | Practical dietary and activity changes; consideration of newer weight-management and glucose-lowering therapies where appropriate. |
| Diabetes & kidney disease | Coordination with your GP, endocrinologist or nephrologist so cardiovascular protection is built into overall management. |
| Lifestyle | Smoking cessation, alcohol, sleep and exercise — addressed specifically, not as an afterthought. |
For practical starting points, see our guides on how to prevent a heart attack and lowering triglycerides, or the 2026 ACC/AHA dyslipidaemia guideline summary for clinicians.
Does preventive cardiology always mean medication?
No. The recommendation depends on your overall risk and the likely benefit of treatment. Some patients may initially need practical lifestyle changes and planned reassessment. Others may benefit from treatment of cholesterol, blood pressure, diabetes or weight-related risk. When medication is recommended, the purpose, expected benefit, possible adverse effects and alternatives are clearly discussed.
Prevention also does not end once coronary plaque has been identified. For people with an elevated calcium score, CT-detected plaque or established cardiovascular disease, prevention usually becomes more intensive, because the underlying risk is better established.
The goal is not to reduce every result to the lowest possible number. It is to reduce the likelihood of heart attack and stroke safely and proportionately.
Preventive cardiology with Dr Reza Moazzeni

Dr Reza Moazzeni is a consultant cardiologist with particular interests in preventive cardiology, inherited lipid disorders and advanced cardiac imaging. His approach combines evidence-based risk assessment with clear, individualised recommendations and close communication with each patient's GP. Consultations are available in English and Persian (Farsi).
Working with your GP
Preventive cardiology works best as a partnership. Your GP remains central to ongoing care: after each consultation your GP receives a detailed letter with the risk assessment, targets and treatment rationale, so prescriptions, repeat pathology and routine monitoring can continue locally. A referral from your GP is required for all consultations, and consultations are privately billed with a Medicare rebate.
Consultation locations
Westmead
Level 3, Office 33
163–171 Hawkesbury Road
Westmead NSW 2145
Serving Western Sydney and Parramatta · Westmead clinic details
St Leonards
Consulting rooms in St Leonards, on Sydney's Lower North Shore.
Echocardiography and stress echocardiography are performed on site at Westmead — see our echocardiogram service page.
Frequently asked questions
Do I need a referral for a preventive cardiology consultation?
Yes. A referral from your GP (or another specialist) is required, and it also enables your Medicare rebate.
What is Lp(a) and why is it measured only once?
Lipoprotein(a) is an inherited cholesterol particle that raises heart attack and stroke risk independently of LDL. Because levels are largely genetically determined, a single measurement is usually sufficient for a lifetime.
Should I have a coronary calcium score?
Not everyone benefits. It is most useful in selected asymptomatic adults with intermediate or uncertain risk, where the result can genuinely change the decision about starting or deferring medication. This is discussed individually at consultation.
I feel well — is a preventive review still worthwhile?
Feeling well does not exclude silent risk. Cardiovascular disease can develop over many years without symptoms, which is precisely why structured risk assessment exists.
Will I definitely be started on medication?
No. Recommendations depend on your overall risk and may include lifestyle measures, surveillance, treatment of cholesterol or blood pressure, or additional investigation. Medication is recommended when the likely benefit justifies it, and the reasoning is discussed with you.
What should I bring to the appointment?
Your referral, any recent blood tests and imaging reports, a list of current medications, and details of your family's cardiac history if known.
This service is intended for planned cardiovascular assessment. If you have severe or persistent chest pain, sudden breathlessness, collapse or other potentially urgent symptoms, call Triple Zero (000) or attend an emergency department.
Book a preventive cardiology consultation
Consultations at Westmead and St Leonards. GP referral required.
Book an appointmentGPs: for urgent cases, use the urgent cardiac referral form.