Coronary artery calcium, or CAC score, is one of the most useful tools for estimating the future risk of a heart attack in the right patient. In this comprehensive guide, I discuss when to consider a calcium score, how to interpret the results, when it can be misleading, and how it fits alongside newer tools like PREVENT, Lp(a) and ApoB in modern cardiovascular risk assessment.

For the broader guideline context, see our 2026 dyslipidemia guideline summary. To estimate your baseline risk, try the PREVENT calculator.
Understanding cardiovascular risk: PREVENT, traditional risk factors, and where CAC fits
Key concept: A coronary calcium score is a risk-refinement tool — not a universal screening test. It is most useful after baseline risk has been estimated, when the result may change how aggressively prevention is approached.
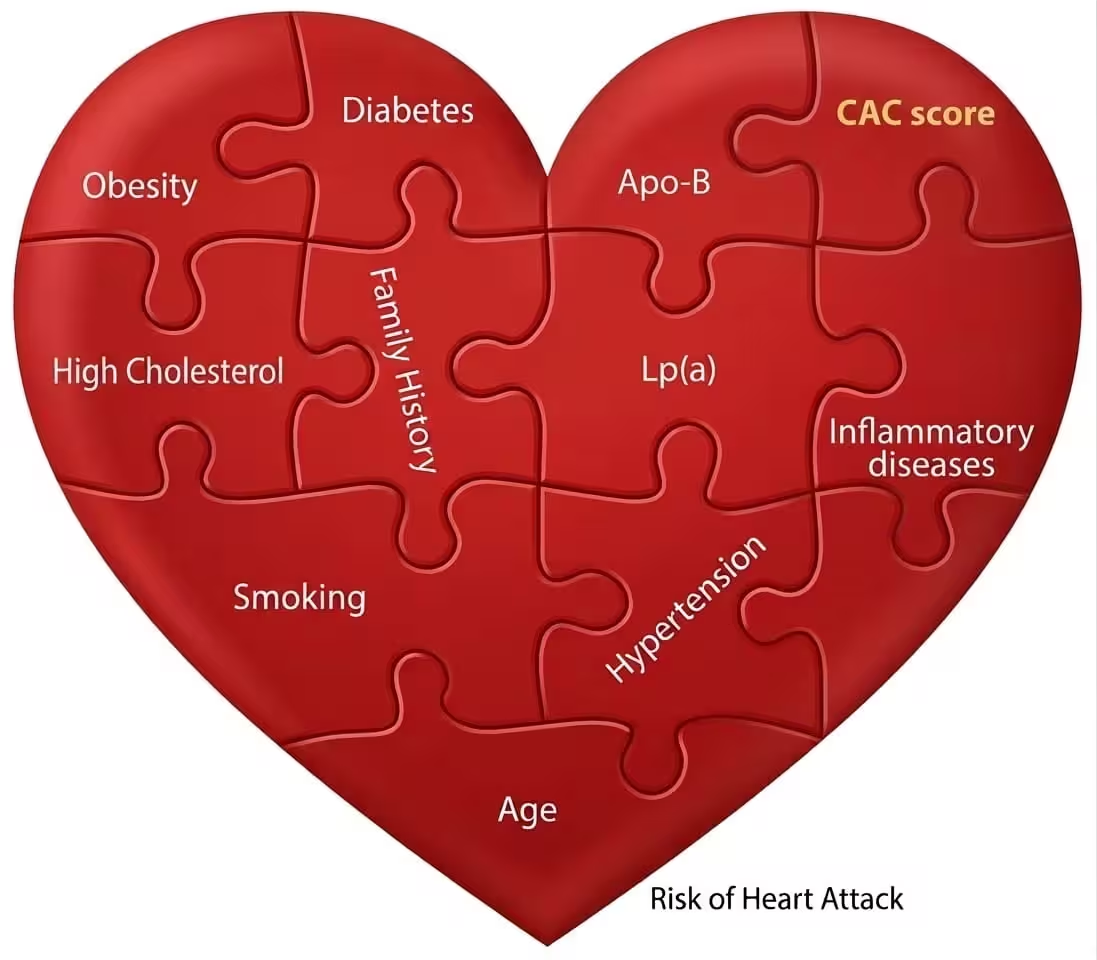
Traditional cardiovascular risk factors still matter: age, sex, smoking, blood pressure, diabetes, cholesterol levels, weight, physical activity, family history, and chronic inflammatory conditions all influence the risk of future cardiovascular disease.
For people without known cardiovascular disease, the starting point is usually a formal risk estimate. The PREVENT risk model is now the preferred framework for primary prevention risk assessment, replacing older ASCVD calculators that used different thresholds. The 2026 ACC/AHA dyslipidemia guideline formally positions PREVENT as the recommended tool in adults aged 30–79 years.
How to interpret baseline risk
Limitations of online risk calculators
Even good calculators can miss important parts of the story. They may underestimate risk in people with a strong family history, elevated Lp(a), inherited lipid disorders such as familial hypercholesterolaemia, or a higher-than-expected burden of atherogenic particles. This is why modern risk assessment increasingly combines traditional risk calculation with additional tools such as Lp(a), ApoB, and coronary calcium scoring when needed.
What is the coronary calcium score (heart calcium test)?
Coronary plaques are the primary precursors of myocardial infarction. The driver behind plaque formation in the arterial wall is atherosclerosis, an inflammatory process that typically starts at a young age. Based on the presence or absence of calcium, plaques are classified as "soft" or "calcified." Initially they are soft and have no detectable calcium, but calcification develops within the plaques over time.
A coronary calcium score is a non-invasive CT scan that measures the amount of calcium deposited in calcified plaques in the coronary arteries. It quantifies calcium deposits and calculates a score. The higher the score, the higher the risk of future cardiac events and stroke. A CAC scan does not show the full biology of plaque, but it gives a practical measure of whether atherosclerosis has already become established and calcified.

Who should have a CAC test?
It is important to understand that a CAC test is not appropriate for everyone. The key principle is simple: CAC is most valuable when the result would change what you do next.
CAC is most useful in:
- Asymptomatic adults with borderline or intermediate estimated cardiovascular risk
- People whose treatment decision is uncertain — especially when deciding whether to start or intensify lipid-lowering therapy
- Adults with risk factors that do not fully explain the clinical picture, such as a strong family history, elevated Lp(a), familial hypercholesterolaemia, or discordance between LDL-C and overall perceived risk
CAC is usually not helpful in:
- Clearly high-risk patients — intensive prevention is already indicated regardless of the score
- Symptomatic patients — the question is no longer risk prediction but diagnosis, and tests such as stress echocardiography or CT coronary angiography are more appropriate
- Very low-risk patients — the result is unlikely to change management
A typical scenario where CAC can help
A 55-year-old asymptomatic man has mildly elevated LDL-cholesterol, well-controlled mild hypertension, no smoking history, and no clear reason to think he is high-risk. His estimated risk appears borderline or intermediate on the PREVENT calculator, but he is reluctant to start medication.
He underwent a CAC scan, which returned a score of 300. A calcium score at this level immediately moves him from borderline to high-risk territory. He is no longer just someone with "borderline numbers" — he is someone with demonstrable coronary atherosclerosis. More intensive LDL-C lowering is now clearly justified, typically aiming for targets consistent with the 2026 dyslipidemia guideline (convert between units here).
On the other hand, if his score had been zero, that would support a more individualised discussion — provided there are no major risk enhancers such as very high LDL-C, familial hypercholesterolaemia, diabetes, or markedly elevated Lp(a).

When should you consider checking your calcium score?
Practical guide: CAC is generally most informative in adults aged approximately 45–75 years, when the decision about preventive treatment is uncertain and the result would influence whether to start or intensify therapy.
In younger adults
A score of zero can be misleading in younger people because CAC detects calcified plaque, not soft plaque. There often has not been enough time for lipid-rich plaques to calcify. A younger patient with familial hypercholesterolaemia, elevated Lp(a), or other inherited risk may still have significant atherosclerosis even if the calcium score is zero. On the other hand, a high score in a young person is highly concerning and should always be taken seriously.
In older adults
Some degree of coronary calcification becomes increasingly common with age, so the absolute score should not always be interpreted in isolation. In older patients, the age- and sex-adjusted percentile often adds useful context — you can check this using our coronary calcium risk calculator. A very low or zero score in an older person can be genuinely reassuring, while a high score should be interpreted alongside the overall clinical picture, including lipid profile, ApoB, Lp(a), and other risk factors.
How to interpret coronary calcium score results
A calcium score should never be interpreted in isolation. The result needs to be considered alongside age, sex, blood pressure, lipid profile, family history, smoking, diabetes, Lp(a), and sometimes ApoB.
No detectable calcified plaque. Reassuring, with low near-term risk — but does not exclude soft plaque, especially in younger people or those with diabetes, smoking, FH, or elevated Lp(a).
Mild calcified plaque and higher risk than a score of zero. Management depends on the broader clinical context — lipid levels, family history, and whether risk-enhancing factors such as Lp(a) are present.
Substantial plaque burden. Usually supports more intensive prevention: lifestyle modifications, risk-factor management, and lipid-lowering therapy guided by the 2026 guideline.
Large burden of coronary atherosclerosis. Budoff et al. (2023) found that patients with CAC >300 had equivalent event rates to those with established ASCVD — suggesting this level should be treated with similar intensity to secondary prevention.

How CAC fits into modern risk assessment
The logic chain: Different tools answer different questions. Used together, they give a much clearer picture than any single test alone.
These tools are complementary. CAC is especially useful when there is uncertainty after the initial clinical assessment, or when the clinician and patient are unsure how aggressive prevention should be. The 2026 ACC/AHA dyslipidemia guideline explicitly positions selective CAC use as part of a broader framework that also includes Lp(a) measurement and ApoB in selected patients.
Putting these pieces together — risk estimation, inherited markers, particle counts, and imaging — gives a much clearer picture than any single test alone. That is exactly the kind of integrated assessment done in a preventive cardiology review.
Coronary calcium in athletes: myths vs realities
Bottom line: Mild coronary calcification in endurance athletes is not uncommon and does not necessarily signal heightened cardiovascular risk. Stable, calcified plaque is different from the dangerous soft plaque that causes heart attacks.
A 2017 study in Circulation examined lifelong endurance athletes and found a higher prevalence of coronary calcification compared to more sedentary individuals; however, much of their plaque was "stable and calcified" rather than the more dangerous "soft and mixed" plaque implicated in acute events such as heart attacks.
While the presence of any calcification may raise concern, overall risk can still be relatively low in athletes who maintain healthy lifestyles and lack other major risk factors — such as significantly elevated LDL-C, high Lp(a), or a strong family history of premature heart disease. If calcification is detected, regular follow-up and personalised medical advice are essential. However, many such individuals with mild calcification can maintain their exercise routines without worrying about negative outcomes.
Limitations of the coronary calcium score test
Calcium scoring is a valuable tool for assessing the risk of coronary artery disease. However, it is not an appropriate diagnostic approach for high-risk patients or those presenting with cardiac symptoms.
Inability to detect soft, non-calcified plaque
The CAC test measures calcified plaque but provides no information about soft, non-calcified plaque. Soft plaques are more prone to rupture and can cause acute coronary events, such as heart attacks.

Potential for false reassurance
In high-risk patients or those with symptoms, a low or zero calcium score can be falsely reassuring, leading to medication non-adherence and a false sense of well-being.
⚠️ Don't over-rely on a calcium score of zero
44-year-old man, smoker, hypercholesterolaemia, strong family history of premature IHD. Presented with chest pain, had a "satisfactory" stress test and a CAC score of zero — reassured. Persistent symptoms led to CTCA, which revealed a significant mid-LAD stenosis, confirmed on invasive angiography (no calcium present, hence CAC 0).
📍 CAC = 0 lowers risk on a population level but does not rule out obstructive disease in high-risk individuals. Use clinical context first.
No functional assessment
The CAC test detects calcified plaques but cannot tell whether those plaques have obstructed the coronary artery — its "functional status." It is possible for an individual to have a high calcium score but still have sufficient blood flow to the heart muscle (non-obstructive plaques) or vice versa. Additional diagnostic tests such as stress testing or coronary angiography may be necessary to evaluate the functional impact of identified calcifications.
Real-life example
A 37-year-old man presents with shortness of breath and throat pain during exertion. Despite having significant traditional risk factors (hypertension, high cholesterol, prediabetes, and a sedentary lifestyle), a CT calcium score was ordered, which was 0. Unfortunately, this led to a false sense of reassurance, and he avoided medical therapy.
Due to persistent symptoms, further evaluation with a stress echocardiogram and CT coronary angiogram revealed a severe blockage in the left anterior descending (LAD) artery, which required a stent placement.


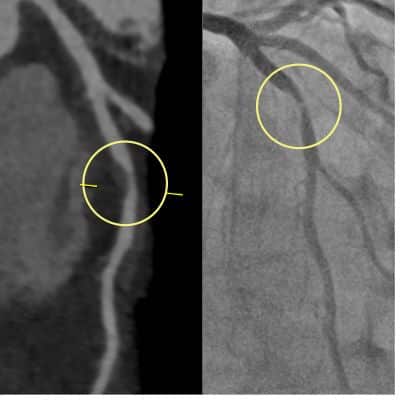
What is the difference between a CT calcium score and a CT coronary angiogram (CTCA)?
While the calcium score is a risk assessment tool, CTCA is a diagnostic test that uses contrast dye to evaluate blood flow and identify narrowing or blockages in the coronary arteries.
CTCA is indicated for patients with symptoms suggestive of coronary artery disease — such as chest pain or breathlessness on exertion — abnormal stress echocardiogram results, or for pre-operative evaluation in certain cases. It provides detailed images of the coronary arteries but involves higher radiation exposure and the use of contrast dye.
In contrast, the calcium score quantifies calcified plaque burden without using contrast dye. It aids in risk stratification but lacks information about non-calcified plaque or blood flow impairment.

Why not just do a CTCA instead?
While CTCA provides more information, there are good reasons to choose a CAC score alone in the right setting: lower radiation exposure (important in younger patients), no contrast dye (relevant for kidney dysfunction or contrast allergy), lower cost (especially for screening in low-to-intermediate risk patients), and avoidance of overdiagnosis — finding "bystander" blockages that may lead to unnecessary anxiety, additional testing, or invasive procedures. The preferred approach for treating asymptomatic coronary disease is intensive medical therapy and healthy lifestyle, and the CAC score is one tool in the box for risk assessment.
In symptomatic patients or those with high-risk features, a CTCA is the more appropriate test. The choice between CAC and CTCA should be based on the patient's individual risk factors, symptoms, and clinical judgement.
Frequently asked questions
The calcium score test is a non-invasive CT scan that takes approximately 10 minutes. It does not require any special preparation, contrast dye, or needles. You lie on a scanning table while the CT acquires images of your heart during a brief breath-hold. The cost varies depending on the location and provider.
A calcium score of 0 is considered optimal, indicating no detectable calcified plaque in the coronary arteries. However, a zero score should be interpreted alongside other risk factors such as age, cholesterol levels, family history, Lp(a), and diabetes — it does not rule out soft non-calcified plaque.
No. Once coronary artery calcification has occurred, it is generally irreversible. However, you can significantly lower your overall risk of cardiovascular events by managing modifiable risk factors — quitting smoking, adopting a healthy diet, regular physical activity, managing stress, controlling blood pressure and diabetes, and taking prescribed medications.
It is worth noting that your calcium score may increase after starting statin therapy or incorporating regular exercise. This is not necessarily a negative development — it may indicate that plaques are hardening and becoming more stable, which can actually reduce the risk of a heart attack.
Generally no, if you are taking your medication regularly and your LDL-C is well controlled. However, if adherence is inconsistent or LDL-C remains significantly above target, a CAC test may help guide the conversation about intensifying therapy. A high score would support a stricter approach; a zero or very low score may support a more individualised discussion about treatment intensity.
Many radiology facilities automatically include calcium scores in CTCA reports, but some may only provide them if specifically requested. To ensure your report contains a calcium score, ask your doctor to order it alongside your CTCA.
If the score is high, repeating the test is generally unnecessary — the focus should be on intensive risk-factor management and lifestyle modifications. Selected patients with a score of zero, especially younger individuals with some risk factors who decided against medication, could consider repeating the test in approximately 5 years.
Conclusion: CAC is one piece of the puzzle
Coronary artery calcium scoring is one of the most useful tools for refining cardiovascular risk in the right patient. It is most helpful in asymptomatic adults when the treatment decision is uncertain and the result would change management.
A high score can reveal that coronary atherosclerosis is already well established and may justify more intensive prevention — particularly aggressive LDL-C lowering. A score of zero can be reassuring, but it should never be interpreted without clinical context, especially in younger adults and in those with inherited risk such as familial hypercholesterolaemia or elevated Lp(a).
In modern preventive cardiology, CAC works best when combined with careful clinical assessment, formal risk estimation with the PREVENT calculator, and selected additional markers such as Lp(a) and ApoB.
- PREVENT cardiovascular risk calculator
- Coronary calcium (MESA CAC) risk calculator
- ApoB calculator and explainer
- Familial hypercholesterolaemia (FH) calculator
- High Lp(a): what it means and what to do next
- Lipoprotein(a): comprehensive review and 2026 update
- 2026 ACC/AHA dyslipidemia guideline summary
References and further reading
- 2026 ACC/AHA clinical practice guideline for the management of blood cholesterol and prevention of ASCVD. J Am Coll Cardiol. 2026.
- Khan SS, et al. Development and validation of the PREVENT equations. Circulation. 2023;148:1982–2004.
- Budoff MJ, et al. Coronary artery calcium scores above 300 equivalent to prior ASCVD for event rates. JACC Cardiovasc Imaging. 2023.
- Greenland P, et al. Coronary artery calcium score combined with Framingham score for risk prediction. JAMA. 2004;291(2):210–215.
- Detrano R, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336–1345.
- Nasir K, et al. Implications of coronary artery calcium testing among statin candidates: MESA. J Am Coll Cardiol. 2015;66(15):1657–1668.
- Yeboah J, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment. JAMA. 2012;308(8):788–795.
- Blaha MJ, et al. Associations between CRP, coronary artery calcium, and cardiovascular events: MESA. Lancet. 2011;378(9792):684–692.
- Merghani A, et al. Prevalence of subclinical coronary artery disease in masters endurance athletes. Circulation. 2017;136(2):126–137.
- Koschinsky ML, et al. Use of Lp(a) in clinical practice: a 2024 focused update from the NLA. J Clin Lipidol. 2024.
