Case presentation

83-year-old man, dual-chamber pacemaker
Progressive exertional dyspnoea and fatigue over three years, with pacemaker-induced severe tricuspid regurgitation on a background of long-standing atrial fibrillation.
History of presenting complaint
An 83-year-old man was referred in 2019 for progressively worsening dyspnoea on exertion and fatigue over the preceding three years. He had no dyspnoea at rest, but his exercise tolerance had declined significantly (NYHA class III), particularly over the previous 12 months. He denied paroxysmal nocturnal dyspnoea or orthopnoea and had no hospital presentations with acute pulmonary oedema — a pattern more consistent with predominant right heart failure. He lived with his partner and remained independent in activities of daily living.
Background
A former professional race-walker, he could comfortably cover 15 km five years earlier but was now struggling to carry groceries from the shops to his car. His only medication was warfarin for long-standing atrial fibrillation, diagnosed in 2000. A permanent pacemaker had been implanted in 2005 for complete heart block. In 2012 he underwent a generator change with insertion of a new ventricular lead; the indication for the new lead was not clear from the available records. An echocardiogram in 2011 showed low-normal left ventricular function, trivial-to-mild tricuspid regurgitation, and a mildly dilated left atrium.
In 2013 — one year after the generator change and new lead — he reported to his cardiologist that "his general health had gone downhill," although he could not elaborate. A repeat echocardiogram at that time showed mild tricuspid regurgitation, mild-to-moderate pulmonary hypertension, and moderately dilated atria. An extended overseas trip then took him out of follow-up for almost five years. His symptoms worsened gradually and were dismissed as "age-related" by family and primary care providers. He had no diabetes, hypertension, or other significant comorbidities, had never smoked, and his renal function was normal.
Physical findings
On presentation in 2019, his blood pressure was 130/70 mmHg and pulse 70 bpm. His chest was mostly clear to auscultation and only mild pitting oedema was present at the ankles. The dominant finding — visible from across the room — was a markedly distended and pulsatile jugular venous pulse, as shown in Video 1.
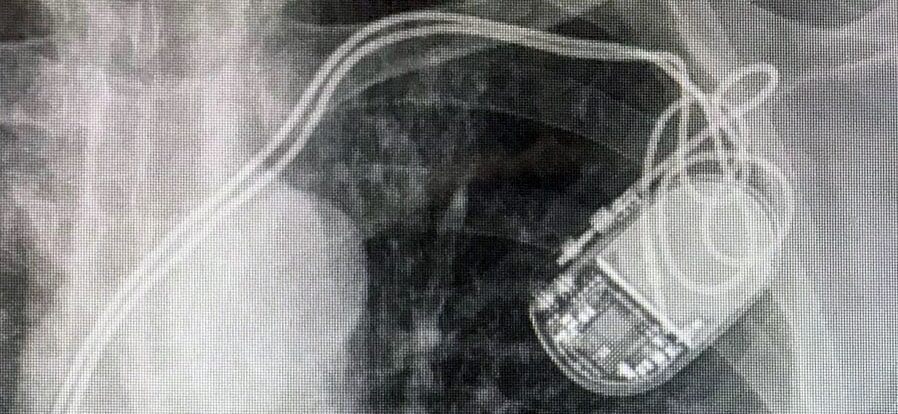
ECG and chest X-ray
The rhythm was paced with underlying atrial fibrillation, with the atrial lead capped. On the PA chest X-ray the right ventricular lead tip lay at the inferior border of the right ventricle; on the lateral view it projected posteriorly — overall consistent with an infero-posterior lead position.



Baseline cardiac function


Tricuspid valve and TR mechanism


