High Lp(a): what it means and what to do next
Lipoprotein(a), or Lp(a), is a type of cholesterol that can quietly raise your risk of heart and blood vessel problems.
High Lp(a) levels have been linked to heart attacks, stroke, valve disease, and even poor circulation in the legs.Doctors have known about Lp(a) for many years, but only in the past couple of decades have we understood how important it is as a separate risk factor — even if your regular cholesterol looks fine.
High Lp(a): what it means and what to do next
Lp(a), or lipoprotein(a), is a genetically determined cholesterol particle that can raise the risk of heart attack, stroke, peripheral artery disease and aortic valve stenosis. Most people with high Lp(a) have no symptoms, so the only way to know is a blood test.
Looking for clinical detail? Read the comprehensive Lp(a) review including emerging therapies, trial updates and the 2026 dyslipidemia guideline summary.
What is Lp(a)?
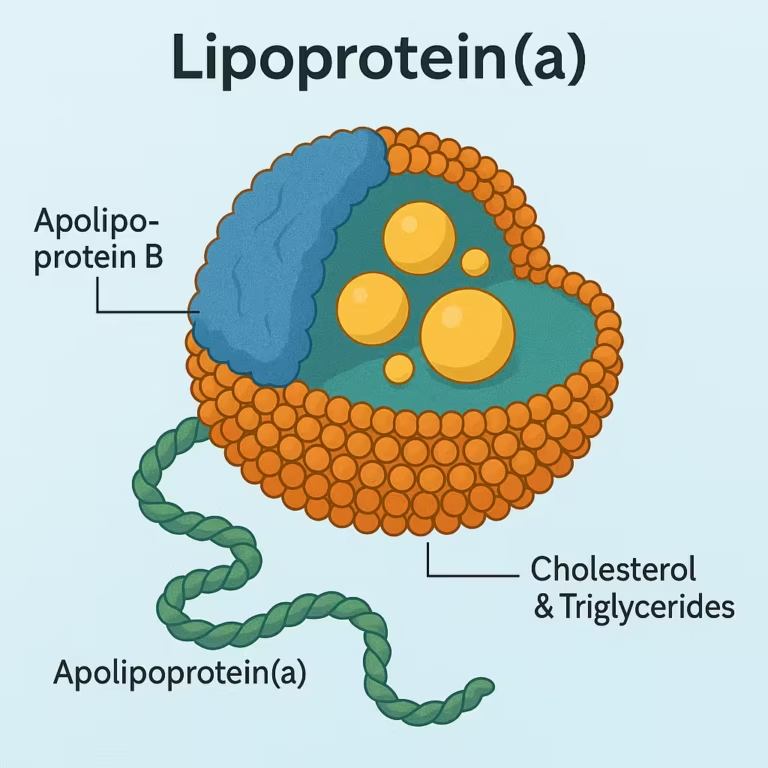
Lipoprotein(a) — often called "Lp little a" — is a cholesterol-carrying particle similar to LDL ("bad cholesterol"), but with an extra protein called apolipoprotein(a) attached. This makes the particle stickier and more likely to contribute to plaque build-up in arteries. Unlike most other cholesterol markers, Lp(a) is overwhelmingly determined by your genes — not by what you eat or how much you exercise. About one in five people has a level that puts them at higher cardiovascular risk, and most of them have no idea.
Who should have an Lp(a) test?
Current guidance — including from the National Lipid Association and the 2026 ACC/AHA dyslipidemia guideline — recommends that every adult have their Lp(a) measured at least once. Because Lp(a) is largely genetic, levels stay stable over a lifetime, so a single test is usually enough.
Testing is especially relevant if you have:
What do my results mean?
Lp(a) is usually reported in nmol/L. Risk increases on a continuum — there is no single number that flips from "safe" to "dangerous" — but the following ranges provide a useful guide:
(<30 mg/dL)
(30–50 mg/dL)
(≥50 mg/dL)
(~100 mg/dL)
Levels around 250 nmol/L (~100 mg/dL) are associated with roughly double the long-term risk of cardiovascular events compared with low levels. Even at intermediate levels, Lp(a) can be a meaningful contributor to overall risk — particularly when other risk factors are present.
What if my Lp(a) is high?
There is no approved medication that specifically lowers Lp(a) yet (though several are in advanced clinical trials). However, a high Lp(a) is not something to simply accept — it means the other factors you can control become more important.
Lp(a) adds risk on top of LDL. Tighter LDL-C targets may be appropriate — discuss with your doctor whether your current therapy is intensive enough.
Blood pressure, diabetes, smoking, weight and physical activity all matter more when Lp(a) is elevated. Every additional risk factor compounds the problem.
A coronary calcium score can show whether plaque has already developed, helping guide how aggressively to treat.
Lp(a) is inherited. First-degree relatives should know their level — a single blood test is all that's needed.
ApoB counts all atherogenic particles, including those carrying Lp(a). It can be more informative than LDL-C alone when risk seems higher than the lipid panel suggests.
Because Lp(a) is genetic, levels rarely change. You do not need to repeat the test unless there is a specific clinical reason.
How do I work out what high Lp(a) means for me?
A single Lp(a) number does not tell the whole story. The impact of elevated Lp(a) depends on your age, sex, blood pressure, cholesterol, diabetes status, kidney function and whether plaque has already developed.
This is where modern risk tools become useful. The AHA PREVENT calculator estimates your baseline 10- and 30-year cardiovascular risk. If your risk is borderline or intermediate, a coronary artery calcium score can help reclassify your risk — either reassuring you or prompting earlier treatment. If there is a suspicion of inherited high cholesterol, the FH calculator can help structure that assessment.
Putting these pieces together — Lp(a), PREVENT score, calcium score, ApoB — gives a much clearer picture than any single test alone. That is exactly the kind of assessment we do in a preventive cardiology review.
When should I see a cardiologist?
Consider a cardiology consultation if you have an elevated Lp(a) together with any of the following: a strong family history of heart disease or stroke, high or difficult-to-treat cholesterol, a coronary calcium score that needs interpretation, uncertainty about whether to start or intensify statin therapy, or known familial hypercholesterolaemia.
A preventive cardiology review brings together your Lp(a) result, lipid profile, risk scores and imaging to build a clear, personalised management plan.
- Lp(a) is largely genetic — you cannot diet or exercise it away
- One blood test is usually enough — levels stay stable over a lifetime
- High Lp(a) means more aggressive management of the risk factors you can control, especially LDL-C
- New targeted Lp(a) therapies are in advanced clinical trials, with results expected from 2026
- Family screening is recommended — first-degree relatives should know their level
Frequently asked questions
Major guidelines now recommend that every adult have their Lp(a) measured at least once in their lifetime. Because Lp(a) is largely genetic and does not change much over time, a single test gives you a lifetime answer. Testing is especially important if you have a family history of early heart disease, known high cholesterol, or are making decisions about statin therapy.
No. Unlike LDL cholesterol or triglycerides, Lp(a) levels are determined almost entirely by genetics. Diet, exercise and weight loss have minimal effect on Lp(a). That is why management focuses on reducing the other risk factors you can control — particularly LDL-C, blood pressure and smoking.
Not yet approved, but several targeted therapies are in advanced clinical trials. These include injectable treatments such as pelacarsen, olpasiran and lepodisiran, which have shown reductions in Lp(a) levels of 80–94% in earlier-phase studies. Major outcome trials are expected to report results in 2026–2029 and will determine whether lowering Lp(a) directly reduces heart attacks and strokes. Read more in our comprehensive Lp(a) review.
Yes. Because Lp(a) is inherited, first-degree relatives — parents, siblings, children — of someone with elevated Lp(a) have a higher probability of also having high levels. A single blood test for each family member can clarify their risk. If you also have a family pattern of high cholesterol, the FH calculator can help determine whether formal assessment for familial hypercholesterolaemia is warranted.
- Estimate your overall risk with the PREVENT calculator The guideline-recommended tool for 10- and 30-year cardiovascular risk
- See whether a coronary calcium score may help Useful when your risk is borderline or you want to reclassify up or down
- Check for familial hypercholesterolaemia with our FH calculator Inherited high cholesterol often coexists with high Lp(a)
- Learn what ApoB measures and how it differs from LDL-C ApoB counts total atherogenic particles — helpful when LDL-C may underestimate risk
- Read our full Lp(a) clinical review In-depth coverage of genetics, pathophysiology, emerging therapies and trial updates
- 2026 ACC/AHA dyslipidemia guideline summary How Lp(a) fits into the latest framework alongside PREVENT, CAC and ApoB