Cardiac masses are uncommon but clinically important — they can embolise to the brain and cause stroke, often in patients with no other conventional cardiovascular risk. Echocardiography is the first-line imaging test for detecting, characterising, and guiding management of cardiac masses. The two cases below illustrate opposite ends of the spectrum: a benign primary cardiac tumour in a young man presenting with palpitations, and a metastatic malignancy in an older patient presenting with stroke.
What These Cases Illustrate
- Cardiac masses can be primary (benign or malignant) or metastatic
- Not every intracardiac mass is a tumour — thrombus and vegetation are important differentials
- Presentation is often non-specific: palpitations, embolic stroke, or incidental finding
- Echocardiography detects and characterises most cardiac masses
- Surgical resection is curative in benign primary tumours such as myxoma
- Metastatic cardiac involvement almost always signals advanced systemic disease
Background on Cardiac Masses
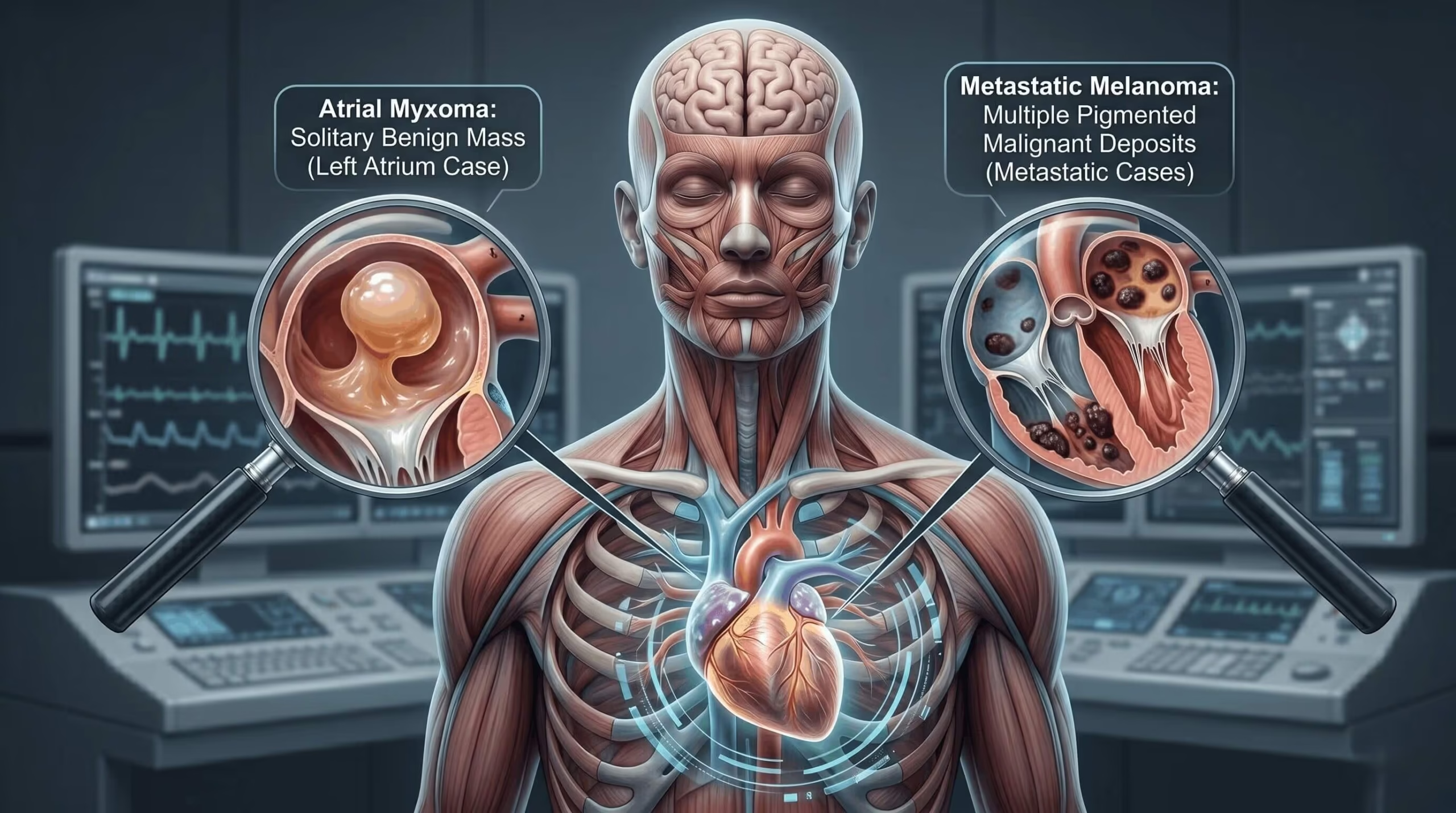
Primary cardiac tumours are rare, with an autopsy prevalence of less than 0.1%. Around 75% of primary tumours are benign — most commonly myxoma. Metastatic involvement of the heart is 20–40 times more common than primary malignancy; lung, breast, melanoma, and lymphoma account for most cardiac metastases.
Cardiac masses broadly fall into four groups: benign primary tumours (myxoma, papillary fibroelastoma, rhabdomyoma, fibroma); malignant primary tumours (angiosarcoma, rhabdomyosarcoma, primary cardiac lymphoma — all rare); metastatic lesions from extracardiac malignancy; and non-neoplastic mimics such as intracardiac thrombus and infective vegetation. Thrombus and vegetation deserve particular emphasis — in everyday practice, they are among the most common causes of an apparent "cardiac mass" on echocardiography, and distinguishing them from true neoplasm is often the clinical task at hand.
- Cryptogenic stroke, particularly in a patient with no atrial fibrillation and no significant carotid disease
- Constitutional symptoms — fever, weight loss, fatigue — classically described with myxoma
- Position-dependent symptoms — dyspnoea or syncope worsening with posture (pedunculated mobile masses)
- Known extracardiac malignancy in a patient with new cardiac symptoms
- Non-specific palpitations or a new murmur in an otherwise healthy young patient
Transthoracic echocardiography is the initial modality in almost all cases. Transoesophageal echocardiography adds detail where TTE is inconclusive, particularly for small masses, attachment points, and prosthetic valves. CT and cardiac MRI provide complementary tissue characterisation when differential diagnosis remains open. For a broader view of echo in stroke workup, see our article on echocardiography in stroke evaluation.
Case 1 — Left Atrial Myxoma in a 38-Year-Old Man
Presentation
A 38-year-old man with no significant medical history presented with a several-week history of palpitations. There was no history of syncope, embolic events, or constitutional symptoms. Cardiovascular examination was unremarkable. Resting ECG showed sinus rhythm, and routine bloods were normal.
Echocardiographic Findings
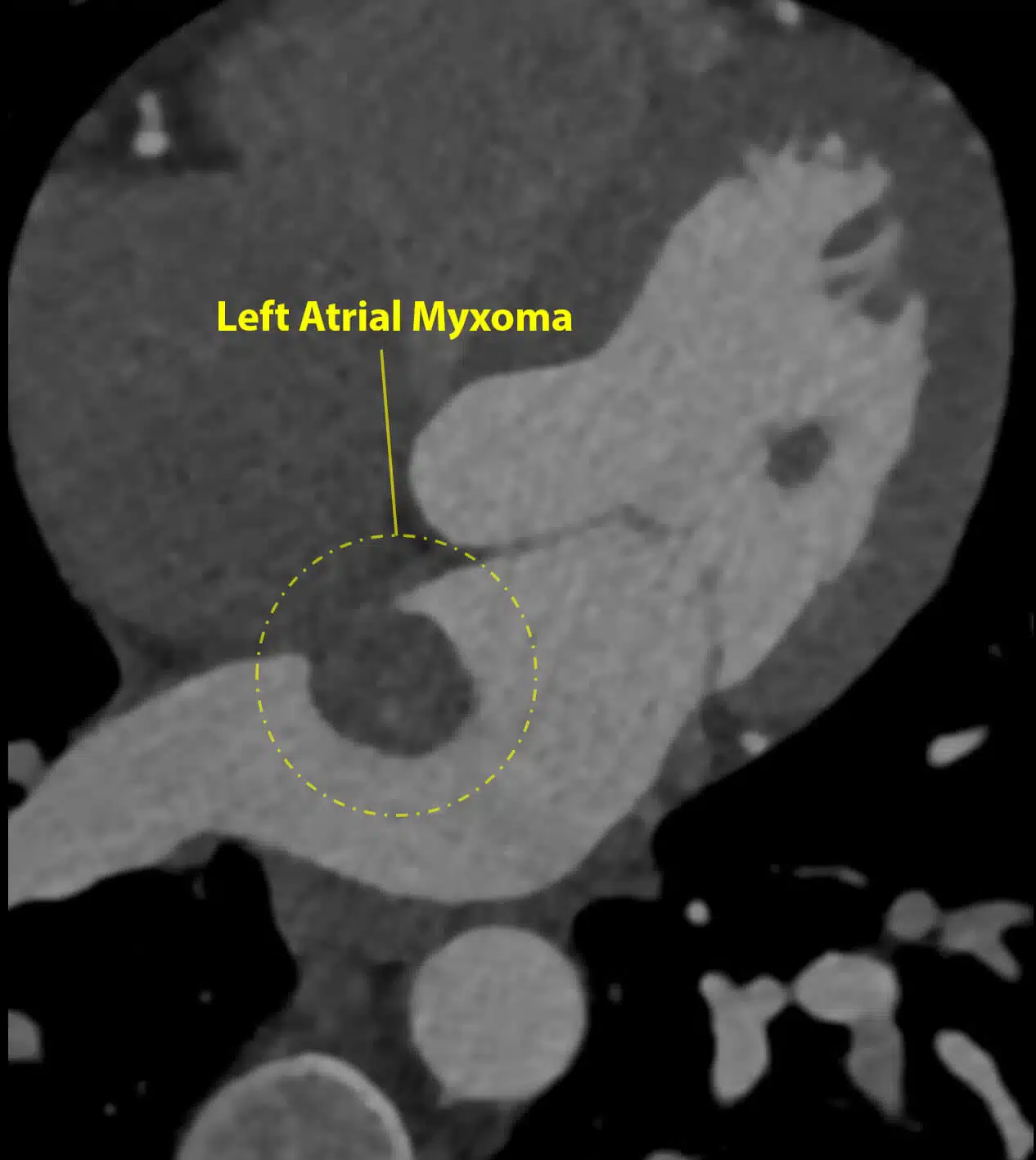
Transthoracic echocardiography revealed a large, mobile mass in the left atrium, attached to the atrial wall by a discrete stalk. Several loosely attached fragments were visible at the surface of the mass, raising immediate concern for embolic risk. Left ventricular size and function were normal; there was no significant valvular disease.
Further Imaging
A CT coronary angiogram was performed to exclude concomitant coronary disease prior to surgery and to better delineate the mass attachment.
Surgical Management
Given the high embolic risk from the mobile fragments, the patient was referred for urgent surgical resection. The mass was removed en bloc along with its attachment site on the atrial wall. The specimen was fragile and required careful handling to avoid fragmentation during excision.

Pathology and Outcome
Histopathology confirmed a benign atrial myxoma. Post-operative recovery was seamless and without complications. Surveillance echocardiography at 6 and 12 months showed no evidence of recurrence.
- Myxoma is the most common primary cardiac tumour in adults, typically arising in the left atrium from the interatrial septum near the fossa ovalis
- Presentation is variable — embolic events, obstructive symptoms (dyspnoea, syncope), or constitutional symptoms (the classical "myxoma triad")
- Palpitations alone, as in this case, are an atypical but recognised presentation
- Surgical resection is curative in the overwhelming majority; recurrence rate is under 5%
- Surveillance echo is recommended post-operatively, particularly in familial (Carney complex) cases
